|
Home | Search | Browse | About IPO | Staff | Links |
|
Home | Search | Browse | About IPO | Staff | Links |
|
By ANTHONY MAN
Tuberculosis not dead
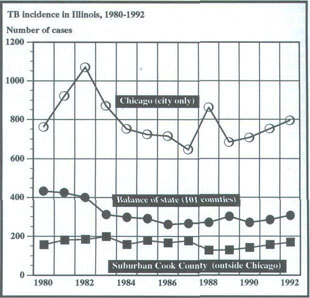
Public health policymakers put to work on ways to handle highly contagious and new drug-resistent TB Tuberculosis is back. Actually it never went away, despite the widespread belief that the once-feared disease is a thing of the past. While TB has been ignored for most of the last decade or two, the public health community now regrets that attitude and wants to reverse it. "It is a very major threat to society at this time," said Dr. Lanie E. Eagleton. He is chief of pulmonary medicine at Southern Illinois University Medical School in Springfield, past president of the American Lung Association of Illinois, and part of a group attempting to put together a state response to the problem. Dr. Agnes D. Lattimer, medical director of Cook County Hospital, called TB "an imminent threat to the health of the entire community." The numbers help show why Eagleton and Lattimer are concerned. Since the mid-1980s, cases have been increasing in Illinois and in the United States. Last year, 1,270 cases were reported to the Illinois Department of Public Health, a 6.5 percent increase from 1991. In the first six weeks of 1993, Lattimer said there were 27 cases of active TB at Cook County Hospital, a 42 percent increase from the same period a year earlier. Although the majority of the state's cases occur in Chicago, the problem is growing everywhere in Illinois. (For TB incidence in Illinois from 1980 through 1992, see graph on page 22.) The resurgence is particularly troublesome because it is marked by a virulent form of the disease that is resistant to standard drug therapy. Drug-resistant tuberculosis is still rare in Illinois. Ben Atkinson, chief of the TB control section at the Department of Public Health, said he determined that 12 percent of last year's most infectious cases were resistant to at least one anti-TB drug, and 1.7 percent were resistant to more than one drug.
July 1993/Illinois Issues/21 areas, and sanitariums where sufferers were sent were closed. Many Illinois counties dropped their TB levies, or used the money for other health-related, but not TB, purposes. Other health developments, such as AIDS, and sociological trends, such as homelessness and immigration patterns, caught up with that lack of concern. The confluence of these trends an increase in the kinds of people susceptible and an increase in the number of people who are in the types of places where the disease can be easily spread means an increase in the number of TB cases. Disproportionate numbers are occurring among the homeless, people with AIDS and the foreign-born. Places like urban homeless shelters, where many people live in close quarters, can be perfect settings for the spread of TB. Delia Mitchell, an organizer for the Chicago Coalition for the Homeless, said shelters are overcrowded and often have bad ventilation. "They're breeding grounds for TB," she said. People with AIDS have impaired immune systems, making them particularly susceptible to a disease like tuberculosis. The federal Centers for Disease Control and Prevention (CDC) estimates that 24 percent of new cases occur in immigrants from countries with a high incidence of TB. Health care workers are also at risk, particularly those who work in hospital emergency rooms in cities with a high incidence of TB. There have been outbreaks among the staff at Cook County Hospital. Others with special risk are people who live in close quarters in institutions such as prisons and nursing homes, the elderly whose immune systems are failing, people who are addicted to drugs and alcohol, people with other diseases such as diabetes, and children since they have immature immune systems. The resurgence of TB and the phenomenon of the drug-resistant variety create a host of health and political issues. To help resolve those problems, a committee has quietly been meeting within the Department of Public Health. The group includes representatives from Cook County Hospital, the city of Chicago, medical schools, the field of pulmonary medicine and the health agency's regulatory and laboratory staffs. Atkinson said the panel soon would start making recommendations to agency director Dr. John Lumpkin, who then may ask the legislature to change state law. Health authorities are considering, and ultimately elected officials may have to wrestle with, the conflict between the individual TB patient's rights and the interests of society. In the past, society's needs were considered paramount. Today's public health authorities are keenly aware of the required balancing act. Lumpkin himself said the things that might be necessary to protect the public health include steps "that we used to consider abhorrent."
22/July 1993/Illinois Issues treatment. With treatment, most cases of normal tuberculosis become noncontagious after a few weeks, even if cure requires years of additional therapy. Failure to complete the course of medication may make the disease go into remission, but the bug is not eradicated in the patient's body. The remaining germs can return in the form that is resistant to anti-TB drugs. Another policy issue involves a small number of people who refuse to cooperate with treatment. The Department of Public Health committee in Illinois and health authorities elsewhere are considering the extent to which people who do not take their medication should be confined to protect the public from exposure. The cost per individual would be high, although the total numbers would not. Though extreme, Atkinson said it is necessary in some cases to prevent infection of others. "If you make the choice not to be medicated, you give up your privilege of living in the community." Eagleton said people cannot be forced to take medicine. However, he said isolation of those who refuse to take medication is reasonable. Unlike the situation decades ago when TB was more prevalent, confinement in the 1990s raises questions of due process and whether those patients should get lawyers and hearings. One question Lumpkin wants answered by his agency's review is whether decades-old anti-TB laws are sufficient for public health authorities to implement rules broad enough to meet today's problems. "Those old laws have never been tested in court," he said. Atkinson said more authority from the legislature is almost certainly needed. "Our ability to function in that area is weak at best."
He said policymakers need to know that "early action is very important." And Lattimer, the Cook County Hospital medical director, said the high incidence in groups that are not politically popular or powerful should not be allowed to cause complacence. "Although it may seem to be limited to the poor and the homeless, that is not true. Children attending school and people riding the bus and train have tuberculosis, and they are potentially exposures for all," Lattimer warned. The legislature has taken one step. Senate bill 846, sponsored by Sen. Judy Baar Topinka (R-22, Riverside), passed the Senate and House unanimously and is awaiting Gov. Jim Edgar's signature. It would require the existing kindergarten, fifth grade and ninth grade school health examinations to include TB tests for children in areas that the Department of Public Health identifies as having a high incidence of the disease. The legislation is aimed primarily at certain parts of Chicago and is designed to uncover families with the disease and get them treatment before the disease spreads. Margaret Fortman, a nurse and TB program coordinator of Chicago Health Outreach, said without more attention, the problem will not stay confined to the groups where it is currently most severe. "Homeless people have families, they go back and forth between shelter and family, they travel all around the city. They ride your buses. They stay in hospitals that you stay in. So when they have TB, TB can be spread all over the city and then all over the state." Anthony Man is Statehouse bureau chief for the four Lee Enterprises newspapers with Illinois readers. He writes frequently about health care.
July 1993/Illinois Issues/23 |
|
|